- Hari ini 28 Nov. genaplah 7 tahun ku hidup sebagai pemandiri kanser. Pada 28 N0v 2006 Jam 2.00 petang ku menjalalni pembedahan gastrectomy and Spleenctomy iaitu membuang separuh daripada perut dan semua limpa kerana sudah merebak dengan sel kanser.
- Sebenarnya berdasarkan CT-Scan, sel kanser dah merebak 2 cm ke hati tetapi doktor tidak usik kerana mereka ragu-ragu sama ada kanser atau bukan.
- Setelah 8 jam di bilik bedah, ku dimasukkan ke ICU sehari dan di tahan di wad pembedahan selama 2 minggu. Seminggu tak dapat makan, cuma bergantung kepada susu yang dimasukkan melalui saluran darah melalui tiub di dada(TPM).
- Hari ke-2 selepas pembedahan ku menjalani x-ray. Sejenis cecair dimasukan melalui tiub dihidung dan gambar pergerakan cecair dapt dilihat melalui skrin komputer. Tubuhku dipusing-pusing untuk memastikan tidak berlaku kebocoran pembedahan.
- Setelah 2 minggu di wad, ku minta kebenaran pulang kerana kedua orang tuaku hendak mengerjakan haji. Sepatutnya ku ikut serta tetapi terpaksa ditunda kerana sakit.
- Januari 2007 ku pergi mengajar sepert biasa tetapi tidak diberi tugas yang berat. Ku letak jawatan segai guru kanan dan menjadi guru biasa saja.
- Mei 2007 ku muntah darah dan diamsukkan ke wad. Seorang doktor melayu berusaha mendapatkan ubat kimoterapi kepadaku yang berharga Rm8380.00 sbeulan. Sebenarnya ku telah berjumpa dengan pakar onkologi sebelum ini tetapi disebabkan kos ubat yang mahal, perkara itu terhenti di situ.
- Kisah lanjut hidup sebagaoi pemandiri kanser banyuk dalam intri ku sebelum ini, folower boleh baca entri 2008 dan 2009.
- Kini ku makan ubat kimoterapi bernama Sutent. Kesan sampingannya sangat teruk, ku tidak dapat berjalan dengan baik kerana tapak kaki ku sakit dan selera makan berkurangan kerana deria rasa di lidah sudah kurang akibat kimoterapi.
- Sekian. Moga para pesakit kanser tabah menghadapi hidup. Insya Allah.
Thursday, November 28, 2013
Ulang tahun ke-7 Sebagai Pemandiri Kanser (Cancer Survivor)
Wednesday, September 11, 2013
Jangan tunggu hingga lapar
Oleh Norlaila Hamima Jamaluddin(harian metro)
Selepas pembedahan pembuangan benjolan di payudara (lumpektomi), teman baik penulis dihujani pelbagai pantang larang makan. Khuatir luka pembedahan akan terasa gatal, ada yang melarang teman ini mengambil ikan dan ayam. Telur dan makanan laut secara automatik masuk dalam kategori ‘diharamkan’.
Masyarakat kita memang murah hati untuk berkongsi pengetahuan dalam soal pantang larang begini, walaupun ada kalanya mereka sendiri tidak pasti apatah pengetahuan yang dimiliki itu benar-benar bermanfaat kerana kebanyakannya diperoleh daripada sumber kurang sahih atau berdasarkan ‘cakap orang’.
Penulis teringat kata-kata doktor yang merawat ibu saudara (ketika dia menjalani kemoterapi akibat kanser usus), supaya memenuhi keinginan selera pesakit kerana mereka amat memerlukan makanan untuk memberi tenaga dan membantu badan memberi tindak balas positif terhadap rawatan.
Saranan dan larangan dalam bab makan seperti inilah yang membuatkan ramai pesakit kanser keliru. Sudahlah pesakit berasa sedih dan susah hati dengan penyakit yang dihidapi, kita yang kurang pengetahuan ini pula membebankan lagi fikiran mereka dengan pelbagai ‘nasihat’ yang belum terbukti keberkesanannya.
Saranan dan larangan dalam bab makan seperti inilah yang membuatkan ramai pesakit kanser keliru. Sudahlah pesakit berasa sedih dan susah hati dengan penyakit yang dihidapi, kita yang kurang pengetahuan ini pula membebankan lagi fikiran mereka dengan pelbagai ‘nasihat’ yang belum terbukti keberkesanannya.
Pengambilan makanan yang berkhasiat dan seimbang amat penting ketika mengharungi saat getir ini. Rawatan kanser seperti pembedahan, kemoterapi dan radioterapi sebenarnya meningkatkan keperluan badan untuk tenaga dan protein. Untuk sembuh dan mengekalkan pertahanan badan terhadap jangkitan, pesakit memerlukan khasiat secukupnya.
Namun rawatan ini ada kesan sampingan kerana ia sedikit sebanyak menjejaskan selera dan pe-ngambilan makanan. Inilah sebabnya doktor yang merawat ibu saudara penulis memberikan nasihat begitu. Malah jika diperhatikan semua doktor dan jururawat memberikan nasihat sama pada kebanyakan pesakit termasuklah wanita yang melahirkan anak. Tentu saja nasihat ini ada pengecualian, contohnya pada pesakit yang menghidap kencing manis, gout, tekanan darah tinggi dan ada masalah jantung.
Memang diakui keba-nyakan pesakit hilang selera makan sepanjang rawatan kanser. Sesetengah rawatan membuatkan mulut pesakit terasa pahit untuk menelan makanan. Walaupun anda tidak berselera, tetapi berusahalah untuk makan supaya badan mendapat khasiat yang diperlukan.
Jangan tunggu hingga berasa lapar untuk makan. Jika sebelum ini anda makan tiga kali sehari, namun pada tempoh penting ini anda dinasihatkan untuk meningkatkan kekerapan makan kepada lima atau enam kali. Makanlah walaupun sedikit dan pilihlah makanan yang berkalori tinggi kerana badan amat memerlukan tenaga untuk melawan penyakit.
Badan kita memerlukan pemakanan sihat untuk berfungsi dengan baik. Ia menjadi lebih penting jika anda menghidap kanser. Pengambilan makanan yang baik ketika menjalani rawatan boleh membantu anda:
Apa yang perlu dimakan?
Pengambilan makanan yang baik bermakna makanan anda perlulah pelbagai berdasarkan Piramid Makanan Malaysia. Ia akan memberikan anda semua khasiat yang badan perlukan untuk melindungi kesihatan ketika anda berjuang melawan kanser. Pemilihan makanan yang sihat akan membantu mempercepatkan proses penyembuhan.
Berikut adalah sembilan panduan untuk pemakanan sihat dan berkhasiat:
Tangani masalah makan
Berdasarkan maklumat daripada buku kecil ‘I Have Breast Cancer. What Next?’ dihasilkan Jabatan Kejururawatan Hospital Assunta untuk pesakit kanser payudara, rawatan kanser memang mempunyai kesan sampingan yang menyebabkan masalah untuk makan.
Untuk mengatasinya, berbincanglah dengan pakar pemakanan di hospital anda mendapatkan rawatan terutama jika tidak pasti apa yang boleh diambil sepanjang rawatan.
Berikut adalah beberapa panduan untuk menangani masalah yang biasa dihadapi oleh pesakit kanser:
a. Berlaku perubahan pada sensitiviti terhadap bau dan rasa
b. Hilang selera makan
c. Sakit mulut atau tekak
d. Mual dan muntah
e. Mulut kering
f. Terlalu kerap buang air besar
Keselamatan
Pada masa sama, anda juga perlu menitikberatkan soal keselamatan kerana sepanjang tempoh mendapat rawatan, badan pesakit kanser amat lemah dan sangat mudah mendapat jangkitan. Inilah sebabnya anda (dan ahli keluarga) perlu memastikan aspek kebersihan diberi keutamaan dalam penyediaan makanan.
Mengambil makanan yang tercemar boleh menyebabkan anda bertambah sakit. Berikut beberapa panduan untuk membantu anda menjaga keselamatan makanan.
Perlukah mengambil makanan tambahan?
Memang ramai pesakit keliru dalam soal ini. Tidak kira berapa banyak pun saranan yang anda terima, berbincanglah dengan doktor terlebih dulu sebelum mengambil sebarang makanan tambahan. Ini kerana sesetengah produk herba didapati boleh mengganggu kesan rawatan kanser.
Malah pakar perubatan juga berbelah bahagi untuk membenarkan pesakit mengambil antioksidan seperti vitamin E kerana ia ada risiko buruk jika berlebihan. Jadi jika anda bimbang mengalami masalah tidak cukup zat, jumpalah pakar pemakanan di hospital bagi mendapatkan khidmat nasihat.
Akhir sekali, jangan lupa untuk melakukan senaman. Apapun bentuk senaman yang anda pilih, semuanya amat berguna untuk membantu anda mengekalkan jisim otot, stamina, kekuatan fizikal dan tulang. Senaman juga dapat membantu mengurangkan kemurungan, tekanan, keletihan, mual dan masalah sembelit di samping merangsang selera makan.
Mulakan dengan senaman yang ringan seperti berjalan selama 10 hingga 15 minit sehari. Apabila anda rasa lebih sihat dan kuat, bolehlah panjangkan tempoh senaman kepada 20 minit sehari. Dengarlah rintihan badan anda dan berhenti apabila dirasakan perlu. Buatlah senaman mengikut kemampuan supaya anda boleh rasa lebih tenang dan bertenaga.
Sunday, September 8, 2013
Sunday, August 18, 2013
Tukar Ubat Lagi
- 15 Ogos 2013, hari raya ke-8, ku ditemani isteri ke klinik Oncologi
- di klink berjumpa dengan kawan senasib, dia datang jumpa Dr.Murali dan ku berjumpa Prof.Biswal. Dia nampak sihat. Dia kata ambil biji aprikot tapi ku masih tunggu dan lihat untuk mengambilnya.
- Ku berjumpa Pof.Biswal. Timbangan beratku 56kg. Dia lihat fistula ku(bisul) yang masih belum sembuh.
- Ku tergagap-gagap bercakap Inggeris dengannya kerana jarang innteraksi dalam bahasa Inggeris, doktor pula tak pandai cakap Melayu walaupun dah lama berkidmat di sini.
- Dia mahu ku buat sekali lagi Pet-Scan kerana ia adalah wajib jika mengambil ubat yang mahal.
- Dia mahu ku berhenti makan Glivec dan mula pula Sutent.
- Selepas 3 bulan, bekalan Sutent akan habis dan dia mahu ku makan pula ubat NEXAVAR(Sorafenib) yang berhaga RM15k hingga RM20K untuk sebulan.
- Ku isi borang permohonan bekalan ubat dari JPA.
- Sebelum pulang, singgah di rumah Ustaz, kawanku di Pulau Melaka, rakan sekerja di SMK Menggatal Sabah dulu. Malu kat dia kerana dia selalu ziarah ku sakit, ku pula sejak sakit dah jarang ke rumahnya.
- Singgah di Maybank Bachok kerana isteri mahu ambil penyata bank.
- Sepanjang perjalanan, asyik terfikir kesan sampingan Naxavar, dr cakap akan muncul jeragat.
- Sekian dulu untuk kali ini. Wassalam.
Sunday, July 28, 2013
Cabaran Bulan Ramadan
- Alhamdulilah sehingga hari ini, dah 19 hari dapat berpuasa tetapi Solat Terawih banyak buat kat rumah kerana tak larat ke surau/masjid.
- Dah lebih separuh Al-Quran dapat dibaca dalam bulan Ramadan ini.
- Hari kedua Ramadan, rumah ku dipecah masuk pencuri, hilang 2 buah laptop. Tahun lepas sehari lepas Nuzul Quran , rumah ku dipecah masuk kali pertama.
- Dah hampir 2 bulan ku minum air rebusan pokok kenerak, ada orang syorkan tetapi masih tidak nampak perubahan.
- Ku masih maka Glivec dan bulan depan akan bertukar kembali ke Sutent. Dr.Biswal cakap dia akan kurangkan dos.
- Semiggu sebelum puasa, warisku kematian anaknya yang baru berusia 12 tahun akibat kanser tulang.
- 17 Ramadan, bekas pengetuaku meninggal kerana leukemia selepas sakit selama 3 tahun.
- Kini ku sudah masuk tahun ke - 8 menghidap kanser perut, moga Allah memberi yang terbaik buat ku di dunia dan akhirat.
- Maaf kerana buat catatan ringkas sahaja kerna hilang mood untuk menulis.
- Selamat Berpuasa.
Wednesday, June 5, 2013
SELAMAT BERSARA.
18 April 2013, ku telah bersara dari menjadi seorang guru. Ku mula berkhidmat sebagai seorang guru pada Jun 1989, lebih dari 23 tahun sebagai guru. Anak sulungku berada di 6 Atas dan anak kedua akan masuk Asasi Sains UIAM pada 8 Jun 2013.
Ku gagahkan diri untuk menghantar anakku ke UIA tetapi orang lainlah yang memandu.
Bisul ku belum sembuh dan kadang-kadang berdenyut-denyut.
Tiba-tiba ku terima panggilan telefon dari sekolah meminta ku menghadiri Majlis Persaraanku sempena Sambutan Hari Guru 2014. Pada mulanya ku tawar hati juga kerana sudah setahun ku pencen baru nak mengadakan majlis, tetapi di sebabkan mereka menggunakan teman baikku menjumputku, ku gagahkan juga pergi ke majlis tersebut walaupun ku sedang makan ubat kimo.
dan kurang sihat.
21 Mei, beberapa orang guru datang menjemput ku di rumah untuk menghadari majlis tersebut. Majlis sambutan ku lihat tidaklah semeriah semasa ku bersekolah dulu kerana PPD mengarahkan sambutan diadakan separuh hari saja. Pun begitu, sekolah menumbangkan seekor lembu sempena majlis tersebut.
Banyuklah juga hadiah yang diberi. Kemudian ku dijemput menghadiri jamuan, ku cuma makan sikit saja kerana banyak yang tak dapat makan.
Beberapa orang guru kemudian menghantarku pulang. Isteriku sebenarnya agak kekok kerana kami tidak menyediakan sebarang jamuan istimewa untuk tetamu kerana isteri bekerja. Ku menenangkan isteri bahawa orang lain bersara kerana tempoh perkhidmatan dah habis, sedangkan saya pencen sakit.
Sekian dulu. Wassalam.
18 April 2013, ku telah bersara dari menjadi seorang guru. Ku mula berkhidmat sebagai seorang guru pada Jun 1989, lebih dari 23 tahun sebagai guru. Anak sulungku berada di 6 Atas dan anak kedua akan masuk Asasi Sains UIAM pada 8 Jun 2013.
Ku gagahkan diri untuk menghantar anakku ke UIA tetapi orang lainlah yang memandu.
Bisul ku belum sembuh dan kadang-kadang berdenyut-denyut.
Tiba-tiba ku terima panggilan telefon dari sekolah meminta ku menghadiri Majlis Persaraanku sempena Sambutan Hari Guru 2014. Pada mulanya ku tawar hati juga kerana sudah setahun ku pencen baru nak mengadakan majlis, tetapi di sebabkan mereka menggunakan teman baikku menjumputku, ku gagahkan juga pergi ke majlis tersebut walaupun ku sedang makan ubat kimo.
dan kurang sihat.
21 Mei, beberapa orang guru datang menjemput ku di rumah untuk menghadari majlis tersebut. Majlis sambutan ku lihat tidaklah semeriah semasa ku bersekolah dulu kerana PPD mengarahkan sambutan diadakan separuh hari saja. Pun begitu, sekolah menumbangkan seekor lembu sempena majlis tersebut.
Banyuklah juga hadiah yang diberi. Kemudian ku dijemput menghadiri jamuan, ku cuma makan sikit saja kerana banyak yang tak dapat makan.
Beberapa orang guru kemudian menghantarku pulang. Isteriku sebenarnya agak kekok kerana kami tidak menyediakan sebarang jamuan istimewa untuk tetamu kerana isteri bekerja. Ku menenangkan isteri bahawa orang lain bersara kerana tempoh perkhidmatan dah habis, sedangkan saya pencen sakit.
Sekian dulu. Wassalam.
Tuesday, February 26, 2013
Kesan Sampingan Glivec
Managing skin side effects from imatinib (Glivec)
Hilary Dearden was diagnosed with a rare type of sarcoma called gastrointestinal stromal tumour (GIST) in her stomach in 2007. She had her stomach completely removed (a total gastrectomy). Fifteen months later the GIST came back in her liver and her cancer specialist started her on imatinib (Glivec). Hilary has taken 400 mg of Glivec once a day for the last 3 years. She tells us about the effects this drug has had on her skin.

My eyes
About a year after I started taking Glivec I noticed a problem with my eyes. They looked all puffy and swollen and I found I couldn’t wear any eye make-up. I happened to mention this to an eye specialist during a routine appointment for my cataract. He suggested that my tear ducts were blocked and thought it could be linked to the Glivec. He recommended using warm compresses. Every day I place 2 cotton wool pads under the hot water tap and then apply them to my eyes, gently rubbing to help clean them. This has helped reduced the swelling and puffiness, although I can still not wear any eye make-up. I also get little bleeds in my eyes.
My face, hair and teeth
Shortly after the problem with my eyes I noticed that I could no longer wear make-up on my face as it made my skin itchy. I have still not found a make-up range I can use so have given up wearing it, but I can use face cream and have found a particular moisturiser that suits my skin I have also had to give up wearing earrings after an episode where my ears turned bright red, swollen and were very painful. I don’t wear much other jewelry, but it does seem to be earrings which are a problem as I can wear a watch with a metal strap with no trouble.
I have little ‘eruptions’ where scabs appear on my face, ears (inside and outside), scalp and shoulders. The scabs tend to develop where my face is bony (like my chin or forehead) or where the skin is thinner. There is never an obvious cause why these scabs have formed. I have not found a way to avoid them but I have learnt to live with them. One of the worse problems is if I catch my tongue on something sharp as it bleeds very easily and will be very sore.
My hair was white prior to starting treatment. After I started the tablets my sister asked me when I had had a pink rinse done and when I checked in the mirror I realised my hair had an orangey ginger tint. My teeth also developed brown stains. The dentist has not been able to treat the staining but I have found a hair dye which I now use to dye my hair blonde and which doesn’t hurt my scalp.
My shoulder
I have a constant itch in just one place, under my left shoulder blade. I don’t know if this is the Glivec or the problem with my liver. When I mentioned it to my cancer specialist he assumed my skin was dry, but I moisturise everyday after my shower and so know this is not the cause. The itch is hard to describe but I would call it an internal itch. Most of the time I forget about it but then I will become conscious of it and have a really good scratch. Unfortunately this is another thing I have learnt to live with.

My lower legs
Of all the areas on my body where I have had problems with my skin the worst place has been my legs, particularly the skin below my knees. About two years ago I fell while looking after my grandson. My knee was in bad way with the skin all scraped off and it was difficult to stop the bleeding. I went to see the district nurse at my GP practice. She treated it with an iodine dressing and then covered the wound with a special plaster. The wound healed within about 10 days and since then every time I have had a really nasty knock I have used the same dressings until it has got better.
My feet
My daughter and I like to go away on city breaks and when we do, I walk the length and breadth of wherever we go. Since being on Glivec my feet tend to develop blood blisters. I always wear comfy shoes and have found rubbing vaseline on my feet, especially between my toes, helps to reduce the risk of blisters forming. My daughter thinks I should try specialist walking socks and so I am going to try some the next time we go away.
On balance
I know I have been lucky with the side effects I have from Glivec and haven’t had the sickness and diarrhoea that I know others have had. My contact with the support group GISTSupport UK has been really invaluable and it is good to be in touch with others who know what you have been going through. Learning how to manage some of these side effects has been a case of trial and error, but I am grateful to be on Glivec, I know if I wasn’t my story might have been very different.
Factfile
- Gastrointestinal stromal tumour is a rare type of sarcoma
- The main treatment is surgery
- Imatinib (Glivec) can be used for a number of reasons, such as GIST that cannot be completely removed, GIST that comes back, or before surgery to shrink GIST and make it easier to remove
- Sunitinib (Sutent) is another type of biological therapy that can be used if Glivec does not work for someone or stops working
More information
On CancerHelp UK there is detailed information about
Sharing your story
The Your tips and stories section of CancerHelp UK provides tips and support for people currently coping with cancer and treatment. You can use the Your tips and stories contribution form to tell us how you coped, so that other people with cancer, or their families, can gain help and support from your stories.
Some people help Cancer Research UK by sharing their stories in other ways – talking to the media, appearing in a Cancer Research UK advert, speaking to volunteers or being featured on our website. Read more about sharing your story.
Rate this page:

- Share this:
- Print this page
 Email this page
Email this page


Monday, February 25, 2013
Kesan Sampingan Ubat Sutent
Prevention and management of hand-foot syndromes

Prevention and management of hand-foot syndromes
HOW TO TAKE THE POST-TEST: To obtain CE credit, please click here after reading the article to take the post-test on myCME.com.
An estimated 1,399,790 new cancer diagnoses were made in the United States in 2006. Most of these cancers required treatment with radiation and/or chemotherapy, interventions that help 65% of persons with cancer to survive at least 5 years after their initial diagnosis.1 The development of novel targeted anticancer agents, such as the tyrosine kinase inhibitors (TKIs)—whether these are used as monotherapy or in combination regimens with chemotherapy—has contributed to improved quality of life and longer survival for cancer patients.1,2 Prolonged survival has in turn underscored the significance of managing emotional, social, and medical problems as integral components of continued cancer care.1
The use of long-term cancer treatments has caused an unexpected constellation of side effects to emerge—most notably the cutaneous toxicities.1 These are becoming more prevalent with increased use of targeted therapies in addition to traditional chemotherapeutic agents.3 Of the cutaneous toxicities experienced by patients, hand-foot syndromes (HFS)—also known as palmar-plantar erythrodysesthesia, palmar-plantar erythema, acral erythema, and Burgdorf's reaction—are becoming among the most common.1-3
Certainly not a new phenomenon, HFS has been reported in 6% to 42% of patients treated with traditional systemic chemotherapeutic agents such as 5-fluorouracil (5-FU, Adrucil,) and its analogs, doxorubicin (Adriamycin, Doxil, Rubex), cytarabine (Cytosar-U, Depo-Cyt), cyclophosphamide (Cytoxan, Neosar), vinorelbine (Navelbine), and docetaxel (Taxotere), as well as in those treated with targeted therapies such as sorafenib (Nexavar) and sunitinib (Sutent).4-10 The incidence of HFS observed in clinical trials with agents such as capecitabine (Xeloda) is around 50%, with 17% of patients reporting a severe form (grade 3).6
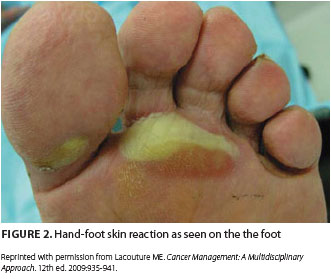
 Adding to this surge of HFS incidence has been the development of novel oral targeted therapies with efficacy against advanced renal cell carcinoma, hepatocellular carcinoma, gastrointestinal stromal tumor, and other tumor types.2,10 These therapies include the TKIs sorafenib and sunitinib, which are notable for causing hand-foot skin reactions (HFSR) in 20% to 40% of treated patients (Figure 1 and Figure 2). HFSR is a distinct variant of the more widely known HFS, which occurs with more traditional chemotherapy agents such as capecitabine.1-4, 10
Adding to this surge of HFS incidence has been the development of novel oral targeted therapies with efficacy against advanced renal cell carcinoma, hepatocellular carcinoma, gastrointestinal stromal tumor, and other tumor types.2,10 These therapies include the TKIs sorafenib and sunitinib, which are notable for causing hand-foot skin reactions (HFSR) in 20% to 40% of treated patients (Figure 1 and Figure 2). HFSR is a distinct variant of the more widely known HFS, which occurs with more traditional chemotherapy agents such as capecitabine.1-4, 10
Although HFS and HFSR do not involve life-threatening toxicities, the syndromes have a significant impact on treatment schedules and quality of life in treated patients.3,5,6Management of HFS and HFSR is geared towards treating symptoms effectively and preventing them from becoming progressive and debilitating.
CLINICAL MANIFESTATIONS
Hand-foot syndrome is a potentially dose-limiting cutaneous toxicity. It is characterized by paresthesia in a sock-and-glove distribution, with varying degrees of pain, tingling, dryness, erythema, scaling, swelling, and vesiculation of the hands and feet.2,8,9 In most instances, symptoms appear after prolonged drug exposure.
 Before the onset of visible symptoms, patients usually experience dysthesia or paresthesia in the palms and soles, including numbness or tingling, which progresses over several days to a burning pain.2,3,6,8-10 Erythema and swelling develop progressively and symmetrically over these areas as well, particularly on the pads of the distal phalanges. Presenting symptoms such as these can interfere with normal activities of daily living. Blisters are more common in areas of great pressure and remain limited to the palms and, less frequently, the soles. HFSR due to TKIs usually manifests as a mild to moderate cutaneous reaction on the hands with a variant pattern, including a form in which bands of erythema alternate with normal skin.2,10
Before the onset of visible symptoms, patients usually experience dysthesia or paresthesia in the palms and soles, including numbness or tingling, which progresses over several days to a burning pain.2,3,6,8-10 Erythema and swelling develop progressively and symmetrically over these areas as well, particularly on the pads of the distal phalanges. Presenting symptoms such as these can interfere with normal activities of daily living. Blisters are more common in areas of great pressure and remain limited to the palms and, less frequently, the soles. HFSR due to TKIs usually manifests as a mild to moderate cutaneous reaction on the hands with a variant pattern, including a form in which bands of erythema alternate with normal skin.2,10
Bullous forms of HFS are more severe and tend to be associated with specific chemotherapy agents such as cisplatin (Platinol-AQ), methotrexate (Trexall), and the TKIs.2,3,5 Some studies have reported that HFSR secondary to TKIs is more likely to manifest as localized patches not only on pressure-bearing aspects of the palms and soles but also on areas that rub against neighboring surfaces, such as the lateral soles and web spaces. HFSR from TKIs can appear within the first 2 to 4 weeks of therapy,2,10 and this occurrence constitutes a variation of HFS distinct from that seen in traditional cytotoxic agents.
PATHOPHYSIOLOGY
Hand-foot syndrome was originally described in 1974 in a patient receiving mitotane (Lysodren).3,4The syndrome was defined again in a 1982 case of a patient receiving a cytarabine-containing chemotherapy regimen and also in 1984 by Lokich and Moore in a phase I study of protracted infusion of fluorouracil. Lokich and Moore described development of a syndrome referred to aspalmar-plantar erythrodysesthesia in 40% or more of the patients. The pathogenesis of HFS is poorly understood, but development of the syndrome appears to be drug-dependent and dose-dependent, with peak plasma drug concentrations, total cumulative dose, and administration schedule affecting the onset and severity.3-5 HFS symptoms may evolve as early as 24 hours after treatment initiation and as late as 10 months after continued therapy.2,3 HFS occurs when small amounts of chemotherapy drug leak out of the capillaries into the hands and feet.11 Once this leak occurs, the drug damages the surrounding tissues.
Previous studies of this syndrome suggest that histologically, the acute erythema of HFS is nonspecific and consistent with a generalized toxicity. Patterns of epidermal cytotoxic injury with mild lymphocyte-predominant dermal infiltrates are described.2,3 Three histopathologic features predominate and are typically associated with traditional chemotherapy-associated HFS and TKI-associated HFSR: dyskeratotic keratinocytes at various stages of necrosis, basal layer vacuolar degeneration, and a mild perivascular or lichenoid lymphocyte-predominant infiltrate.2,9 These histopathologic features of HFS are believed to occur through two mechanisms of action; one is direct toxic effect due to drug exposure, and the other, a new theory unique to the TKIs, suggests that inhibition of both platelet-derived growth factor receptor (PDGFR) and vascular endothelial growth factor receptor (VEGFR) in concert may impede vascular repair mechanisms.2
Direct toxicity The most commonly accepted theory of HFS pathogenesis involves direct toxicity of chemotherapeutic agents against acral epithelium.2,3,6 The most common histopathologic pattern observed—a cell-poor lymphocytic interface dermatitis with basilar vacuolar degeneration, dyskeratosis, and inflammatory changes such as dilated blood vessels, edema, and WBC infiltration—is strongly descriptive of direct toxic mechanisms of injury. Local delivery of high drug concentrations through eccrine (sweat) glands has been implicated in the etiology of HFS induced by chemotherapeutic agents such as doxorubicin and TKIs such as sorafenib.6 Notably, the palms and the soles have the highest concentration of eccrine glands in the body, thus supporting the possibility that drug accumulation in sweat results in particularly high concentrations in acral skin. One study that tested five skin surface areas of a single patient before and after doxorubicin administration demonstrated high levels of drug accumulation in the palms and soles only, and deep within the sweat duct on the palms only, supporting the theory that the drug accumulates differently in the acral areas than in the rest of the body.2,3,6
PDGFR and VEGFR inhibition The association of TKIs with the development of HFSR provides very little evidence to support a direct drug toxicity effect on the eccrine secretion properties of acral surfaces.2 The impediment of vascular repair mechanisms imposed by these agents is believed to play a significant role in the development of HFSR. Deficits of this caliber would be most clinically apparent in areas exposed to high pressure and repeat trauma, such as the palms and soles, where vessels are more likely to be damaged and dependent on intact vascular repair mechanisms.2,3,6,10
CLINICAL ASSESSMENT AND DIAGNOSIS
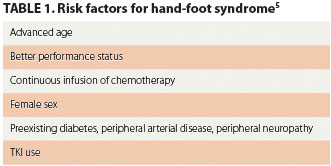 The diagnosis of HFS and HFSR is based on clinical presentation at baseline and after the initiation of therapy. Patients being treated with cytotoxic agents or TKIs that have the potential to induce cutaneous symptoms should be evaluated for such toxicities each time they are examined by a clinician. The assessment should include measures that identify and stratify patients who are at an increased risk for developing HFS and/or HFSR (Table 1).5 The clinical signs and symptoms are distinctive, and diagnosis is based on the presenting symptoms and treatment history.3 Early identification, addressing symptoms, and taking measures to prevent symptoms from worsening are imperative to improving clinical outcomes.
The diagnosis of HFS and HFSR is based on clinical presentation at baseline and after the initiation of therapy. Patients being treated with cytotoxic agents or TKIs that have the potential to induce cutaneous symptoms should be evaluated for such toxicities each time they are examined by a clinician. The assessment should include measures that identify and stratify patients who are at an increased risk for developing HFS and/or HFSR (Table 1).5 The clinical signs and symptoms are distinctive, and diagnosis is based on the presenting symptoms and treatment history.3 Early identification, addressing symptoms, and taking measures to prevent symptoms from worsening are imperative to improving clinical outcomes.
The grading system for HFS and HFSR reflects that increasing duration of exposure to the chemotherapeutic agent or TKI increases the severity of the syndrome.4,8-10 Assessment of symptoms should be graded according to appropriate staging, such as those presented in the criteria listed by the National Cancer Institute's Common Toxicity Criteria, version 4.0. Evidence-based approaches for the prevention and treatment of HFS and HFSR support grading these symptoms to help provide the most effective and appropriate intervention.
PREVENTION AND TREATMENT
The current treatments for hand-foot symptoms are mainly anecdotal. No standard therapies have demonstrated 100% efficacy, but symptom management and evidence-based guidelines have proved to be beneficial in treating patients with HFS and HFSR. Management focuses overall on reducing modifiable risk factors that can worsen symptoms and on preventing or treating symptoms in a timely and effective manner to minimize associated physical and psychosocial discomfort and to ensure uninterrupted antineoplastic therapy.1
Clinicians must become educated about hand-foot syndromes and their implications. In turn, clinicians must educate patients undergoing treatment with cytotoxic agents or TKIs about how to recognize symptoms, along with the importance of notifying health care providers immediately at the first appearance of symptoms.7,10
PREVENTION
According to the American Society of Clinical Oncology (ASCO), patients at risk for HFS and HFSR should be instructed on the following preventive measures:
- Limiting exposure of hands and feet to hot water when washing dishes or bathing
- Taking cool showers or baths
- Avoiding exposure to sources of heat, including saunas, sitting in the sun, or sitting in front of a sunny window
- Avoiding activities that cause unnecessary force or friction on the feet, such as jogging, aerobics, and long walks
- Avoiding contact with harsh chemicals used in laundry detergents or household cleaning products
- Avoiding the use of rubber gloves to clean with hot water, as rubber traps heat against the skin
- Avoiding the use of tools or household items that require pressing the hand against a hard surface, such as garden tools, knives, and screwdrivers.7,11
- A "3C" approach to TKI-associated HFSR outlines the following guidelines for prevention:
- Controlling for calluses: before and during treatment, prophylactic removal of hyperkeratotic areas with a manicure or pedicure
- Comfort with cushions: protection of tender areas, pressure points, and pressure-sensitive areas of the hands and feet through the wearing of well-padded, well-fitted, soft shoes; foam-type absorbing soles, and shock absorbers to relieve painful pressure points
- Cover with creams: use of an emollient or keratolytic agent on callused areas of the palms and soles to moisturize and aid in natural exfoliation.10
TREATMENT
If HFS occurs despite efforts to prevent it, the focus should switch to managing existing symptoms, reducing complications, and preventing symptoms from worsening. Interventions should concentrate on lifestyle changes that avoid aggravation to the hands and feet.1-3,5,7,10 Therapies include dose modification, pyridoxine, regional cooling, celecoxib (Celebrex), topical urea, and oral corticosteroids.
Dose reduction Of all the recommended therapies for treatment of HFS, the most definitive therapy is dose reduction and treatment interruption.2,3,7 Studies show that within 2 to 4 weeks of drug cessation, HFS symptoms resolve. Manufacturer recommendations for TKIs such as sorafenib and sunitinib are to interrupt therapy for any grade 3 HFSR or for any persistent grade 2 HFSR.2 Therapy can resume after the HFSR reaches grade 0 or 1 but at a reduced dosage (sorafenib, 400 mg twice daily reduced to once daily; sunitinib, dose decreases in decrements of 12.5 mg).
Pyridoxine Very few data support the use and efficacy of vitamin B6 in managing the HFSR induced by TKIs. However, many case reports have demonstrated the beneficial effects of pyridoxine in dosages of 50 to 300 mg daily for management of HFS induced by traditional chemotherapeutic agents.2,3,7 Controlled studies have shown that the concomitant administration of pyridoxine delayed onset and reduced the severity of cutaneous toxicities associated with select chemotherapeutic agents (eg, pegylated liposomal doxorubicin).3 A small study (56 patients) reported at the ASCO 2010 Gastrointestinal Cancers Symposium found that among patients being treated with capecitabine, those taking 400 mg of pyridoxine daily had less palmar-plantar erythrodysesthesia than did patients taking 200 mg of pyridoxine daily, suggesting that the higher dose of pyridoxine was the more effective preventive therapy.12 Ongoing clinical trials hope to gain insight into the full benefit of pyridoxine in the clinical setting with regard to managing HFS and its role in HFSR induced by TKIs.
Cyclo-oxygenase-2 inhibitors Retrospective studies have demonstrated that cyclo-oxygenase-2 (COX-2) may help to mediate the inflammatory process that occurs with HFS caused by chemotherapy agents. These studies demonstrated a decreased incidence of HFS in patients treated with capecitabine.2,3 There is limited evidence to support the benefit of COX-2 agents in managing HFSR caused by TKIs.
Vasoconstrictive therapies Modalities such as localized cooling of acral areas to induce vasoconstriction can decrease the amount of drug delivered to these areas.2,3,7
Topical emollients Use of topical emollients, especially those containing lanolin, has proven to be effective in soothing affected areas of skin in HFS or HFSR. The greatest benefit of topical emollients lies in their ability to enhance moisture retention and maintain hydration, thereby reducing further desquamation and decreasing infection risks.10
CONCLUSION
Hand-foot syndromes can impair physical and psychosocial coping in patients undergoing treatment for cancer. Because these disorders can be quite debilitating and greatly compromise quality of life, management must be aggressive and timely. Early intervention is essential to preventing high grades of cutaneous toxicity and consequent treatment disruption. Care and management of HFS must also be multidisciplinary in its approach, and the role of various supportive treatment modalities continues to be investigated in the clinical arena and in clinical trials. Most importantly, educating patients about HFS and HFSR is imperative so that symptoms can be recognized early and toxicities limited. As TKIs continue to be used along with traditional chemotherapy and as new treatments continue to be developed, gaining a better understanding of the pathogenesis of hand-foot syndromes is essential. Effective management of these syndromes is imperative to improve clinical outcomes and preserve the quality of life in our patients. ONA
Jia Conway is an oncology nurse practitioner at Cancer Care Associates of York in York, Pennsylvania, and a member of the Oncology Nurse Advisor editorial board.
HOW TO TAKE THE POST-TEST: To obtain CE credit, please click here after reading the article to take the post-test on myCME.com.
REFERENCES
1. Agha R, Kinahan K, Bennett CL, Lacouture ME. Dermatologic challenges in cancer patients and survivors. Oncology (Williston Park). 2007;21(12):1462-1472.
2. Lipworth AD, Robert C, Zhu AX. Hand-foot syndrome (hand-foot skin reaction, palmar-plantar erythrodysesthesia): focus on sorafenib and sunitinib. Oncology. 2009;77(5):257-271.
3. Scheithauer W, Blum J. Coming to grips with hand-foot syndrome. Insights from clinical trials evaluating capecitabine. Oncology (Williston Park). 2004;18(9):1161-1184.
4. Lokich J. The three most common chemotherapy-related skin reactions. Oncology (Williston Park). 2007;21(12). CancerNetwork Web site. http://www.cancernetwork.com/display/article/10165/63103?pageNumber=1. November 1, 2007. Accessed June 10, 2010.
5. Heo YS, Chang HM, Kim TW, et al. Hand-foot syndrome in patients treated with capecitabine-containing combination chemotherapy. J ClinPharmacol. 2004;44(10):1166-1172.
6. Milano G, Etienne-Grimaldi M, Mari M, et al. Candidate mechanisms for capecitabine-related hand-foot syndrome. Br J Clin Pharmacol. 2008;66(1):88-95.
7. Pike K. Hand-foot syndrome. Oncol Nurs Forum. 2001;28(10):1519-1520.
8. Lee C K, Lynch J. Hand-foot syndrome in breast cancer patients receiving adjuvant chemotherapy.Intern Med J. 2007;37(4):281-282.
9. Bardia A, Loprinzi CL, Goetz MP. Hand-foot syndrome after dose-dense adjuvant chemotherapy for breast cancer: a case series. J Clin Oncol. 2006;24(13);e18-e19.
10. Wood LS, Lemont H, Jatoi A, et al. Practical considerations in the management of hand-foot skin reaction caused by multikinase inhibitors. Commun Oncol. 2010;7(1):23-29.
11. Hand-foot syndrome or palmar-plantar erythodysesthesia. American Society of Clinical Oncology Web site.http://www.cancer.net/patient/All+About+Cancer/Treating+Cancer/Managing+Side+Effects/Hand-Foot+Syndrome+or+Palmar-Plantar+Erythrodysesthesia. June 2009. Accessed June 10, 2010.
12. Chalermchai V, Sriuranpong V. A randomized trial of two different doses of pyridoxine in the prevention of capecitabine-associated palmar-plantar erythrodysesthesia. Abstract 468. American Society of Clinical Oncology 2010 Gastrointestinal Cancers Symposium.http://www.asco.org/ASCOv2/Meetings/Abstracts?&vmview=abst_detail_view&confID=72&abstractID=1262. Accessed June 10, 2010.
HOW TO TAKE THE POST-TEST: To obtain CE credit, please click here after reading the article to take the post-test on myCME.com.
Catatan: Kesan ini ku alami sewaktu memakan Sutent sampai tidak dapat berjalan. Mulut juga mengalami ulcer selain badan terlalu letih.
Subscribe to:
Comments (Atom)